 Posted on May 13, 2025
Posted on May 13, 2025
Seeing Beyond the Surface: The Power of Intravascular Ultrasound (IVUS) in Cardiology
In the ever-evolving field of cardiovascular care, accuracy and clarity can save lives. Traditional angiography has long been the go-to method to visualise blockages in the coronary arteries, but what if we could actually look inside the artery walls—not just at the surface? That’s exactly what Intravascular Ultrasound (IVUS) enables.
IVUS is more than just a fancy imaging tool. It’s a game-changer that allows doctors to see beyond the dye, offering precise and layered insights into coronary artery disease (CAD), stent placement, and complex lesions. If you or someone close to you is dealing with heart disease or undergoing a coronary intervention, understanding IVUS could make all the difference.
What is IVUS?
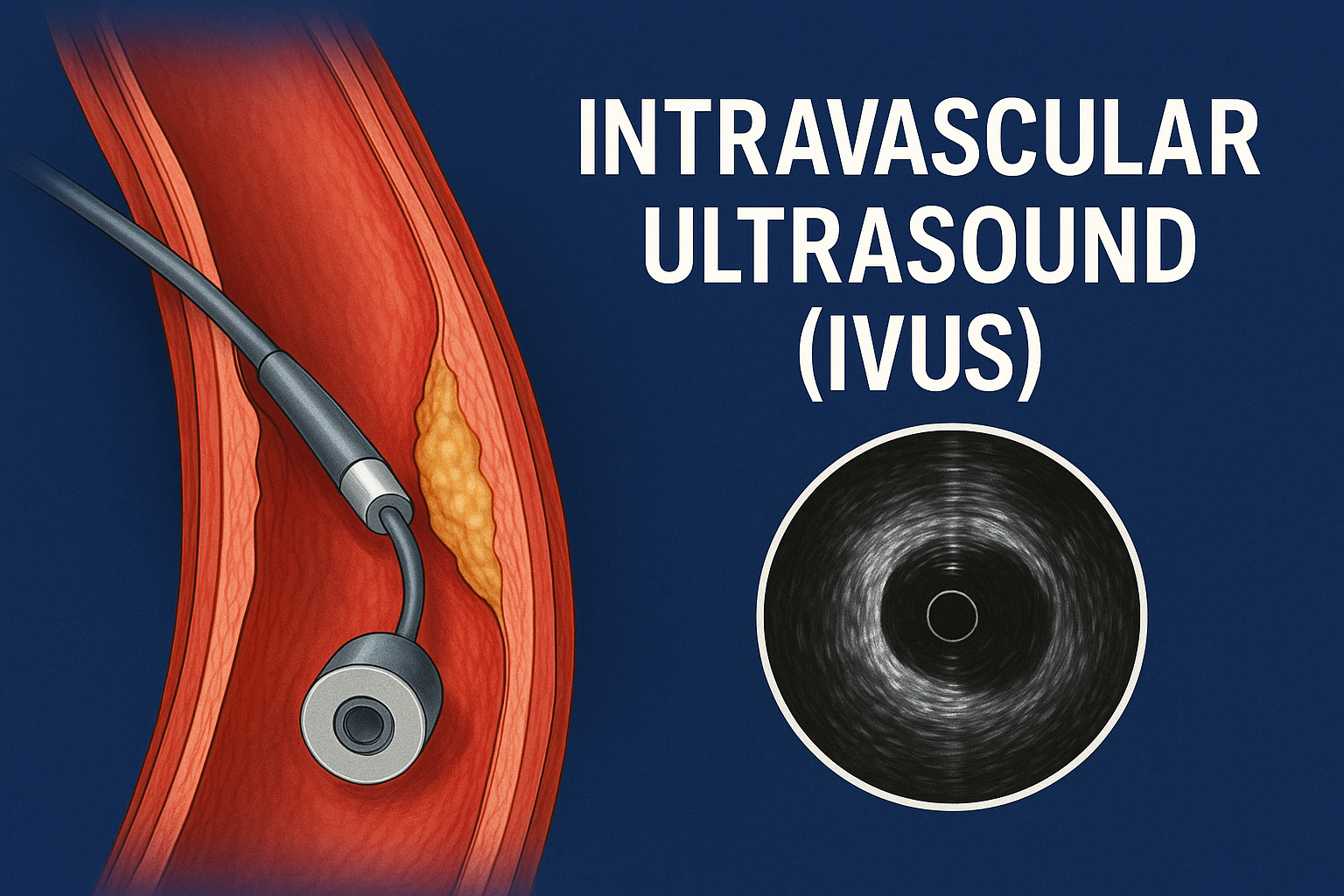
Intravascular Ultrasound (IVUS) is an imaging modality that uses high-frequency sound waves to create a detailed, cross-sectional image of blood vessels from the inside out. Unlike conventional angiography, which shows the outline of arteries using contrast dye and X-rays, IVUS shows the walls of the artery, revealing how much plaque is really there and what kind it is.
An IVUS catheter has a miniaturised ultrasound probe at its tip. Once it’s inserted into the blood vessel (usually during a catheterisation procedure), it emits sound waves that bounce off vessel walls. These echoes are picked up and converted into real-time images.
Why IVUS? What Makes It Special?
While angiography remains the gold standard for diagnosing blockages, it has its limitations:
| Angiography | IVUS |
|---|---|
| Only shows lumen (inner opening) | Shows vessel wall, plaque burden, and size |
| Can underestimate or miss plaque | Detects hidden atherosclerosis |
| Based on 2D images | Gives 360-degree cross-sectional views |
| No tissue characterisation | Detects fibrous, calcific, or soft plaques |
In short, IVUS helps doctors see what angiography can’t.
How Does IVUS Work?
-
Catheter Insertion: A catheter is threaded through the arteries to the heart, often from the femoral or radial artery.
-
Ultrasound Probe Activation: The mini probe at the tip emits high-frequency sound waves.
-
Image Capture: These waves reflect off the vessel walls and tissues.
-
Data Interpretation: The returning echoes are processed to form detailed cross-sectional images on a monitor.
These images can show:
-
Plaque size and type
-
Arterial remodelling
-
Stent expansion and apposition (whether the stent is fully open and in contact with the vessel wall)
When is IVUS Used?
IVUS isn’t done routinely for every angiogram, but it’s indispensable in certain cases. It’s often used in:
1. Complex Coronary Artery Disease
When plaque isn’t clearly visible or the artery has mixed disease patterns, IVUS provides clarity. It helps decide whether to stent, and how long/wide the stent should be.
2. Left Main Coronary Artery Disease
This artery supplies a large portion of the heart. Misjudging its blockage can be fatal. IVUS confirms whether intervention is needed, and how much.
3. Stent Optimisation
After a stent is placed, IVUS ensures it’s fully expanded and pressed against the artery wall. This reduces the chances of restenosis (narrowing again) or thrombosis (clot formation).
4. Assessment of Plaque Composition
Knowing whether a plaque is calcific or soft influences treatment. Hard plaques may require rotational atherectomy before stenting.
5. Dissection or Vessel Injury
If there’s a suspected tear or injury during a procedure, IVUS can confirm and guide further management.
Types of IVUS Systems
There are two main types of IVUS systems used in practice:
1. Mechanical IVUS
-
Rotating transducer at the tip
-
Good image quality
-
More susceptible to mechanical issues
2. Electronic IVUS (Phased Array)
-
Uses multiple stationary transducers
-
Faster pullback
-
Less image artefact
Step-by-Step: A Case of IVUS in Action
Let’s walk through a typical case:
Patient: 58-year-old male with diabetes, chest pain, and known coronary artery disease.
Angiogram findings: Moderate narrowing in the left main artery—ambiguous.
What now? IVUS is introduced through the catheter.
Findings with IVUS:
-
Significant plaque burden
-
Positive arterial remodelling
-
Narrow true lumen diameter <4.5 mm²
Decision: Angiogram alone suggested borderline disease, but IVUS proved it was significant. A stent was placed with IVUS guidance, ensuring optimal expansion.
Outcome: Clear flow, reduced risk of complications, and peace of mind for both patient and physician.
Benefits of IVUS
-
✅ Improves accuracy in identifying true severity of blockages
-
✅ Guides stent sizing precisely—avoiding over- or under-sizing
-
✅ Reduces procedural complications
-
✅ Improves long-term outcomes by optimising treatment
-
✅ Essential in complex or ambiguous cases
Limitations of IVUS
While it’s incredibly useful, IVUS does have a few limitations:
-
❌ Not available in all cath labs
-
❌ Adds cost to the procedure
-
❌ Requires trained interpretation
-
❌ Time-consuming in some complex cases
-
❌ Cannot replace angiography—used as an adjunct
IVUS vs. Other Imaging Modalities
| Feature | IVUS | OCT (Optical Coherence Tomography) | Angiography |
|---|---|---|---|
| Imaging Medium | Ultrasound | Light | X-ray (dye) |
| Resolution | Moderate | High | Low |
| Penetration | High | Low | N/A |
| Visualises Vessel Wall | ✅ | ✅ | ❌ |
| Needs Blood Clearance | ❌ | ✅ | ❌ |
| Best For | Plaque burden, calcification | Stent struts, fine structures | Lumen outline |
Summary: IVUS is preferred when deep tissue visualisation is needed. OCT is better for finer structures.
The Future of IVUS
With the rise of AI-enhanced image interpretation, IVUS is becoming smarter and faster. Modern systems can automatically assess:
-
Plaque burden
-
Vessel diameter
-
Need for intervention
Some systems even integrate IVUS with co-registration, overlaying ultrasound images with angiographic views for precise localisation.
Common Questions About IVUS
What does IVUS show that angiography doesn’t?
IVUS shows the actual vessel wall, allowing physicians to see how much plaque is present—even when the artery looks normal on angiography.
Is IVUS safe?
Yes. IVUS is performed during a standard catheter-based procedure. The risks are minimal when done by an experienced team.
How long does an IVUS procedure take?
IVUS adds about 5–10 minutes to a typical coronary procedure but adds immense value in complex cases.
Is IVUS painful?
No. Patients don’t feel the IVUS catheter specifically. It’s done during angiography under sedation or local anaesthesia.
How much does IVUS cost?
Costs vary depending on the hospital and country. It’s often bundled into the total procedure cost, especially in complex angioplasty or stenting cases.
Can IVUS be used in peripheral arteries?
Yes. IVUS is also used in peripheral vascular interventions—for arteries in the legs, renal arteries, and even carotid arteries in certain cases.
Do all stents require IVUS?
Not always. But in complex blockages, left main artery interventions, or repeat procedures, IVUS is strongly recommended to ensure proper stent placement.
📍 Consultation Locations
Dr. Girish B Navasundi
Senior Consultant Interventional Cardiologist & Certified TAVR Specialist
Lead Consultant – Structural Heart Disease & Heart Failure
🏥 Apollo Hospitals
📍 154, Apollo Hospitals, 11, Bannerghatta Rd, Opp. I.I.M,
Amalodbhavi Nagar, Panduranga Nagar, Bengaluru, Karnataka 560076
🕒 Mon – Sat: 10 AM – 4 PM
🏥 Legends Heart Center
📍 1st floor, 37/17, 10th Main Rd, 5th Block, Jayanagar, Bengaluru, Karnataka 560041
🕒 Mon – Sat: 4 PM – 8 PM