 Posted on April 22, 2026
Posted on April 22, 2026
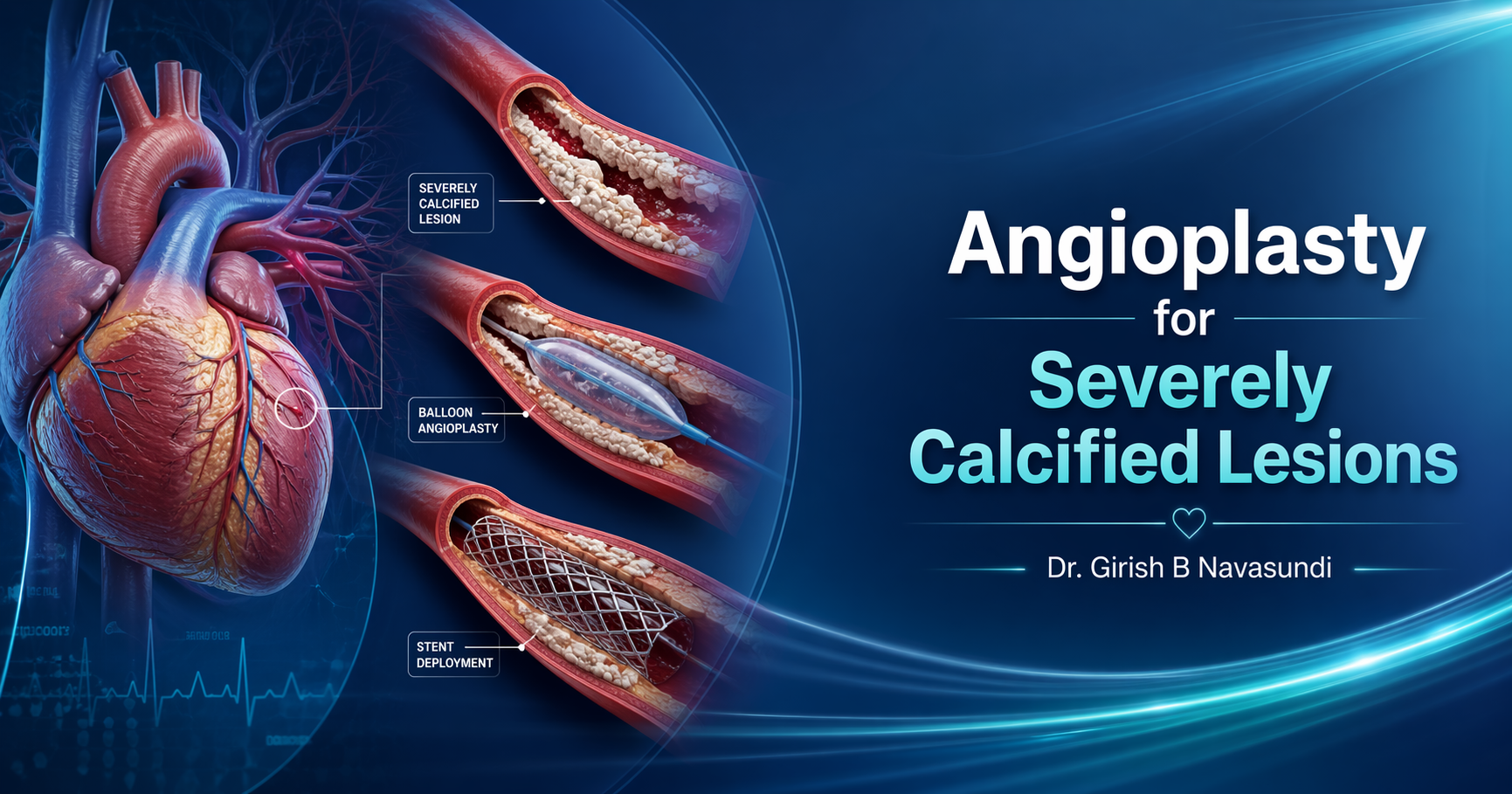
Angioplasty for Severely Calcified Lesions: What Patients and Families Need to Know
When people hear the word angioplasty, they often imagine a blocked artery that can simply be opened with a balloon and treated with a stent. In many cases, that is true. But not all blockages are the same.
Some heart artery blockages are far more complex because they are severely calcified. This means the artery has become hardened by calcium deposits over time, making it rigid, narrowed, and much more difficult to treat. These are not ordinary blockages. They demand planning, precision, experience, and the right technology.
For patients and families, hearing terms like “heavily calcified artery,” “high-risk angioplasty,” or “complex coronary disease” can be overwhelming. It raises immediate questions. Is angioplasty still possible? Is surgery better? Is it dangerous? What does recovery look like? And most importantly, what is the safest path forward?
The good news is that modern interventional cardiology has advanced significantly. Today, many severely calcified lesions can be treated successfully with specialized angioplasty techniques. But these decisions must never be rushed. The goal is not only to open the artery, but to choose the treatment that is safest, most durable, and most appropriate for the patient as a whole.
What does “severely calcified lesion” mean?
A lesion in cardiology refers to a narrowed or blocked part of a coronary artery. When that lesion is calcified, it means calcium has built up within the artery wall over years. This makes the artery stiff and resistant.
Think of a normal soft blockage like a traffic jam that can be pushed aside. A calcified blockage is more like a hardened concrete ring inside the artery. It does not expand easily. It may resist balloons. It may prevent proper stent delivery or expansion. And if not treated correctly, it can affect the long-term success of the procedure.
Severe calcification is more commonly seen in:
- older adults
- people with long-standing diabetes
- patients with chronic kidney disease
- those with high cholesterol or smoking history
- individuals with long-standing coronary artery disease
In such cases, a routine angioplasty approach may not be enough.
Why are calcified coronary lesions more challenging?
Severely calcified lesions create several important challenges.
First, they can make it difficult for the cardiologist to pass equipment through the artery. Even if the blockage can be crossed, the hardened calcium may stop the balloon from expanding properly.
Second, stents need to open fully and sit snugly against the artery wall to work well. In a heavily calcified artery, the stent may remain underexpanded. This is a serious concern because an underexpanded stent may increase the risk of future complications such as re-narrowing or clot formation.
Third, these lesions are often found in patients who may already have more complex heart conditions, including multiple blockages, reduced heart function, or other medical problems. That means the decision is not simply about whether the artery can be opened. It is about whether the full treatment strategy is right for that person.
This is why high-risk or calcified-lesion angioplasty should be approached with careful planning and specialist judgment.
Symptoms that may suggest significant coronary narrowing
Patients with severely calcified lesions may experience the same symptoms seen in other forms of coronary artery disease, including:
- chest pain or chest heaviness
- breathlessness on exertion
- chest discomfort while climbing stairs or walking
- unusual fatigue
- reduced exercise tolerance
- symptoms after meals, emotional stress, or physical activity
In some patients, especially those with diabetes, symptoms may be subtle. Instead of classic chest pain, they may feel tired, short of breath, or unable to do their usual activities.
When symptoms are significant, or when tests suggest high-risk disease, further evaluation becomes important.
How is severe calcification identified?
Coronary angiography may suggest the presence of calcium, but in many cases, specialists use advanced intravascular imaging to understand the blockage more clearly from the inside of the artery.
This helps answer crucial questions:
- How much calcium is present?
- Is the calcium superficial or deep?
- How long is the calcified segment?
- Will a balloon alone be enough?
- Is plaque-modification technology needed before stenting?
This is one of the major reasons why complex angioplasty should be done in experienced hands. A good outcome depends not only on opening the artery, but on choosing the right technique for that exact lesion.
Can angioplasty still be done for severely calcified lesions?
Yes, in many patients, angioplasty is still possible and can be performed successfully. However, it often requires specialized lesion-preparation techniques before a stent is placed.
These techniques are designed to modify or fracture the calcium so the artery can expand more safely and effectively. Depending on the anatomy and the clinical situation, the interventional cardiologist may consider different tools and technologies to prepare the lesion.
The purpose of this preparation is simple: create the best possible environment for optimal stent expansion and long-term success.
Not every patient with severe calcification needs the same approach. That is why personalized planning matters.
Why treatment planning matters so much
One of the biggest misconceptions patients have is that every blockage should automatically be treated with angioplasty. In reality, coronary disease treatment is much more nuanced than that.
A patient may have:
- a single complex calcified lesion
- multiple severe blockages
- left main coronary disease
- reduced heart pumping function
- heart failure symptoms
- valve disease alongside coronary disease
- advanced age or frailty
In such situations, the right question is not just, “Can this artery be opened?” The better question is, “What is the best overall treatment plan for this patient?”
Sometimes that plan may involve angioplasty. In some cases, bypass surgery may be considered. In others, medical management or a staged approach may be more appropriate. What matters is thoughtful decision-making that considers symptoms, anatomy, heart function, age, long-term safety, and quality of life.
What happens during angioplasty for calcified lesions?
The procedure is similar in broad concept to standard angioplasty, but the execution may be far more advanced.
A small catheter is inserted, usually through the wrist or groin, and guided to the heart arteries. The blockage is crossed carefully with specialized wires. The lesion is then assessed and prepared using suitable devices.
After the calcium has been adequately modified, the artery is expanded and a stent may be placed if appropriate. Imaging may again be used to confirm that the stent is fully expanded and well positioned.
This level of precision is especially important in calcified disease because the final result must be mechanically sound. A stent that only looks acceptable on routine angiography may still not be optimal if the calcium has not been properly treated.
Is it a high-risk procedure?
Some calcified-lesion angioplasties are considered high-risk, but that does not mean they should be avoided. It means they should be approached carefully, with the right expertise, preparation, and judgment.
Risk depends on many factors, including:
- where the blockage is located
- how much calcium is present
- whether there are multiple narrowed arteries
- how strong or weak the heart muscle is
- the patient’s kidney function and other medical illnesses
- whether the patient is stable or having an acute heart event
When a procedure is high-risk, experience matters even more. The safest results often come from specialists who routinely evaluate complex coronary disease and who understand when to proceed, when to stage treatment, and when another strategy may be better.
Benefits of treating severely calcified lesions properly
When the right patient is selected and the lesion is treated effectively, angioplasty can offer meaningful benefits.
These may include:
- relief from angina or chest discomfort
- improved blood flow to the heart muscle
- better exercise tolerance
- reduced shortness of breath in selected patients
- improved daily functioning and confidence
- avoidance of ongoing ischemia caused by severe narrowing
But the real benefit lies not just in doing the procedure, but in doing it well. In complex calcified disease, precision is everything.
Recovery after angioplasty
Recovery after angioplasty is usually faster than after open-heart surgery. Many patients are able to go home within a short period, depending on the complexity of the procedure and their overall condition.
After the procedure, patients are typically advised regarding:
- blood-thinning medications
- cholesterol-lowering therapy
- diabetes and blood pressure control
- cardiac rehabilitation where appropriate
- smoking cessation
- heart-healthy diet and activity guidance
- follow-up consultations and symptom review
It is important to remember that angioplasty treats a blockage, but long-term heart care goes beyond the procedure itself. Risk factor control remains essential.
When should you seek a specialist opinion?
A specialist assessment can be especially valuable if you or your loved one has been told:
- there are multiple coronary blockages
- one or more arteries are heavily calcified
- angioplasty may be difficult or high-risk
- surgery has been suggested, but you want to understand all options
- symptoms are continuing despite medicines
- there is concern about age, frailty, or heart function during treatment planning
In these situations, the goal of consultation is clarity. Patients deserve to understand the anatomy, the risk, the available options, and the reasoning behind the recommended treatment.
The importance of individualized decision-making
Severely calcified coronary disease is not a one-size-fits-all problem. Two patients may both have “calcified blockages,” yet require completely different treatment strategies.
That is why an experienced interventional cardiologist looks beyond the angiogram alone. The full picture matters:
- symptoms
- artery anatomy
- heart function
- associated valve or structural heart issues
- age and frailty
- diabetes, kidney disease, and other medical conditions
- long-term goals and expected quality of life
This kind of thoughtful decision-making is especially important in advanced heart conditions. It ensures that the treatment plan is not only technically possible, but genuinely right for the patient.
Final thoughts
Angioplasty for severely calcified lesions is one of the more demanding areas in modern cardiology. These are not routine blockages. They require expertise, careful imaging, advanced lesion preparation, and sound clinical judgment.
For patients, this can feel intimidating. But it should also be reassuring to know that treatment options have evolved significantly. Many complex lesions that once seemed extremely difficult can now be approached with far greater precision than before.
Still, the most important step is not the procedure itself. It is the decision that comes before the procedure. Choosing whether angioplasty is appropriate, how it should be done, and whether it is truly the safest option for that individual is where specialist care makes a real difference.
FAQs on Angioplasty for Severely Calcified Lesions
1. What is a calcified coronary lesion?
A calcified coronary lesion is a blockage in a heart artery that contains hardened calcium deposits. This makes the artery stiff and more difficult to treat than a soft plaque blockage.
2. Is angioplasty possible in heavily calcified arteries?
Yes, in many cases it is possible. However, these procedures often require specialized techniques and careful planning before the artery can be safely stented.
3. Why is calcification a problem during angioplasty?
Calcium can prevent balloons from expanding properly and may stop a stent from opening fully. This can affect both immediate success and long-term results.
4. Is bypass surgery always better for calcified blockages?
Not always. The best treatment depends on the number of blockages, their location, the patient’s age, heart function, symptoms, and overall medical condition.
5. Is calcified-lesion angioplasty considered high-risk?
Some cases are high-risk, especially when there are multiple blockages, weak heart function, or complex artery anatomy. That is why specialist evaluation is important.
6. What symptoms can severely calcified blockages cause?
Common symptoms include chest pain, heaviness, breathlessness, unusual fatigue, and reduced exercise tolerance. Some patients may have subtle symptoms.
7. How long is the recovery after angioplasty?
Recovery is often quicker than with bypass surgery. Many patients recover within a short period, though the exact timeline depends on the complexity of the case and overall health.
8. Can calcified lesions come back after treatment?
Any treated artery needs long-term follow-up, medicines, and risk-factor control. Proper stent expansion and ongoing heart care help reduce future problems.
9. Do all calcified lesions need treatment?
No. Treatment depends on symptoms, severity of narrowing, blood flow impact, and the patient’s overall condition. Not every lesion automatically needs angioplasty.
10. When should I get a second opinion?
A second opinion is especially helpful if you have been told the blockage is complex, severely calcified, high-risk, or if you want clarity between angioplasty, surgery, or medical treatment.
About Dr. Girish B Navasundi
Dr. Girish B Navasundi
Senior Consultant Interventional Cardiologist & Certified TAVR Specialist
Lead Consultant – Structural Heart Disease & Heart Failure
His practice is especially relevant for patients who need thoughtful decision-making in advanced heart conditions—not just whether a blockage can be opened, but whether the full treatment plan is right for the patient’s heart, age, symptoms, and long-term safety.
If you or a loved one has been told there are multiple heart blockages, severe coronary narrowing, or a high-risk angioplasty requirement, a specialist assessment can help clarify the safest next step.
Consultation Locations in Bangalore
Apollo Hospitals
154, Apollo Hospitals, 11, Bannerghatta Rd, Opp. I, I.M, Amalodbhavi Nagar, Panduranga Nagar, Bengaluru, Karnataka 560076
Mon – Sat: 10 AM – 4 PM
Legends Heart Center
1st Floor, 37/17, 10th Main Rd, 5th Block, Jayanagar, Bengaluru, Karnataka 560041
Mon – Sat: 4 PM – 8 PM